This creates a strong attention bias toward the same side as the injury, while the opposite side may be ignored or “neglected.” Because spatial attention networks are larger and more interconnected in the right hemisphere, neglect of the left side after right-brain damage is more common than right-sided neglect after left-brain damage.
They are almost always unaware of their actions, depending on the task, such as reading text messages, locating a house key, or cleaning their face.
Because of damage to the wide-spread ventral and dorsal attention networks, spatial neglect affects multiple perceptual modalities (visual, auditory, tactile, proprioception) as well as multiple cognitive and motor functions. However, there is no gold standard for its screening, comprehensive assessment, and treatment. The main reason lies in the complexity of the syndrome.
The impacts of the disorder are therefore understandable but underappreciated. More than four decades of clinical research has shown that spatial neglect impedes rehabilitation outcomes, increases the risk of falls, prolongs functional recovery, and worsens stress and burden among family caregivers of stroke survivors.

The outlook for individuals with spatial neglect largely hinges on detecting symptoms early. Therefore, the critical first step toward improving outcomes is to identify spatial neglect accurately in individuals who have had a stroke.
Clinical observation and quick tests are essential because individuals with spatial neglect may not always recognize their deficits, making self-reporting unreliable.
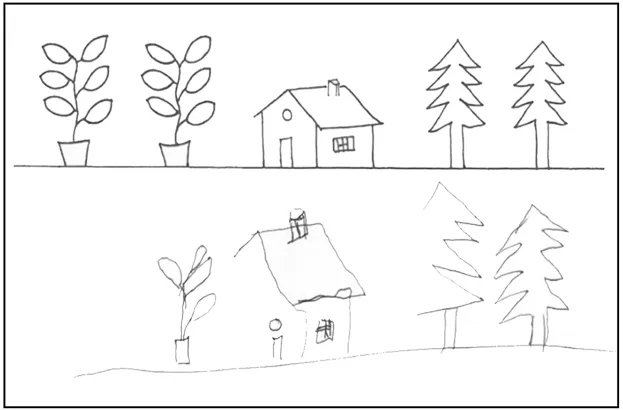
A comprehensive evaluation will clearly identify the symptoms of spatial neglect. This evaluation should include a number of different tests sensitive to various symptoms of spatial neglect (e.g., typical object drawing, figure copying, target cancellation with varied difficulty levels, text reading, extinction in visual, tactile, auditory, and motor modalities) and incorporate at least one ecological assessment like KF-NAP® to measure the extent of functional disability.
Assessments for spatial neglect can be carried out by trained professionals, including neuropsychologists, occupational therapists, physical therapists, speech and language pathologists, neurologists, and other clinical specialists.
A person-centered approach and treatment plan should be created after analyzing different test results and quality of performances with consideration of the individual’s self-awareness deficits.
Neglect Symptoms Vary Across Spatial Regions
Symptoms of spatial neglect can be manifested in different spatial regions, both close to and distant from the body. All the examples below reflect left-sided spatial neglect, but are also applicable to right-sided spatial neglect.
- Personal space (body parts or body surface). For example, an individual might only shave or apply lotion to the right side of their face, leaving the left side largely untouched
- Peri-personal space (within arm’s reach). For example, experiencing difficulty finding utensils on the left side of a food tray
- Extra-personal space (beyond arm’s reach). For example, overlooking furniture or people across the room on the left side
Symptoms can be egocentric (body-centered, viewer-centered) and/or allocentric (stimulus-centered, object-centered). Clinically, egocentric spatial neglect receives more emphasis because it poses a greater disability risk. This form of spatial neglect involves individuals making errors or omissions, specifically on their left side. In contrast, allocentric spatial neglect involves errors on the left side of an object, regardless of its position relative to the individual.

The deficits created disrupt basic self-care activities (e.g., dressing, grooming), impair postural balance, interfere with reading ability, and impede navigation (e.g., avoiding furniture when using a wheelchair, dodging oncoming vehicles when crossing streets).
Many individuals with spatial neglect are unaware of their own symptoms or the consequences of their deficits (i.e., anosognosia), which delays their seeking appropriate treatment or learning compensatory strategies. This self-awareness deficit can jeopardize safety, especially among individuals who have regained some ambulatory ability after stroke.
Below are symptoms most typically observed in individuals by healthcare professionals and clinicians who specialize in neurorehabilitation and disability research. Stroke survivors with left-sided spatial neglect may:
At rest, individuals may naturally look toward the right side, even without external prompts. This rightward bias often lessens when they become actively engaged in a task.
When spoken to face-to-face, they may shift their eyes toward the right rather than maintaining centered eye contact.
If approached from the left, they may turn or respond toward the right instead of orienting toward the person or stimulus on their left.
Posture may be tilted to the right, with the head and eyes turned in that direction. This can make sitting or standing appear off-center.
They may neglect the left arm or leg, leaving a limb unsupported or not use it spontaneously, even after strength and movement have improved.
When reading aloud, they may skip words or phrases located on the left side of text, such as the beginnings of lines or menu items.
Objects on their left may go unnoticed or be hard to locate.
Items may be clustered on their right, with few items placed on the left.
They may bump into objects on the left when moving around.
They may show little concern about issues such as weakness on the left side of their body. This differs from typical denial, where a person may consciously choose to ignore a problem.
They appear unconcerned to difficulties they are having. They may pause during tasks without recognizing or explaining the problem.
According to Kessler Foundation’s research based on data of more than 4,400 individuals (82% of them were stroke survivors) admitted to rehabilitation hospitals, more than 60 percent of stroke survivors have spatial neglect and are in need of effective treatment.
To address these challenges, Center research scientists strive to strike a balance between scientific exploration and practical application. Their studies encompass a range of technologies and approaches, from low-tech prism adaptation treatment equipment to innovative virtual reality and mixed reality methods. The Center team is helping to enhance the knowledge and improve the practice of clinicians worldwide with these tools:
- Kessler Foundation Neglect Assessment Process (KF-NAP®)
- Kessler Foundation Prism Adaptation Treatment (KF-PAT®)
- Kessler Foundation Spatial Re-Training Therapy (KF-SRT®) currently in development
- Kessler Foundation Eye Movement Exercise (KF-EME™) currently in development
Loss of vision in part of the visual field, affecting either half (hemianopia) or one quarter (quadrantanopia) of what a person can see. This sensory problem results from damage to the retina, the primary visual cortex, or the nerve pathways that connect them.
Spatial neglect disrupts how the brain uses visual information but is not a problem with the eyes or basic vision. It is a neuropsychological condition caused by damage to attention networks involving multiple cortical regions, subcortical structures, and connecting white matter pathways.
Oculomotor symptoms in spatial neglect are related to difficulty controlling gaze rather than problems receiving visual information from the eyes. The inability to control gaze or eye movement in many individuals with spatial neglect can affect daily functions that require vision.
Some individuals experience both a visual field cut and spatial neglect, depending on the location and extent of the brain injury.
A visual field cut typically affects vision the same way across activities, causing persistent loss or blurring on one side. Spatial neglect, however, can change depending on the task. A person may groom evenly yet miss the beginnings of sentences when reading, or easily find items on a table but struggle to arrange them correctly.
The severity of spatial neglect may change with alertness, fatigue, cognitive load, or distractions. In contrast, a visual field cut typically remains stable and does not vary much over time or across situations.
The Network for Spatial Neglect promotes accurate detection, direct translation of research to practices, and effective treatments tailored to people with various types of spatial neglect. Provide your contact information to receive updates regarding Kessler Foundation Neglect Assessment Process (KF-NAP®), Kessler Foundation Prism Adaptation Treatment (KF-PAT®), and the Center’s latest studies.
Note: Kessler Foundation is committed to protecting the privacy of its web visitors. Information provided by visitors is not sold to any individual organization.
